
April 2022 Issue
ISSN 2689-291X
ISSN 2689-291X
Aortic Valve Papillary Fibroelastoma:
Source of Embolic Angina!
Description
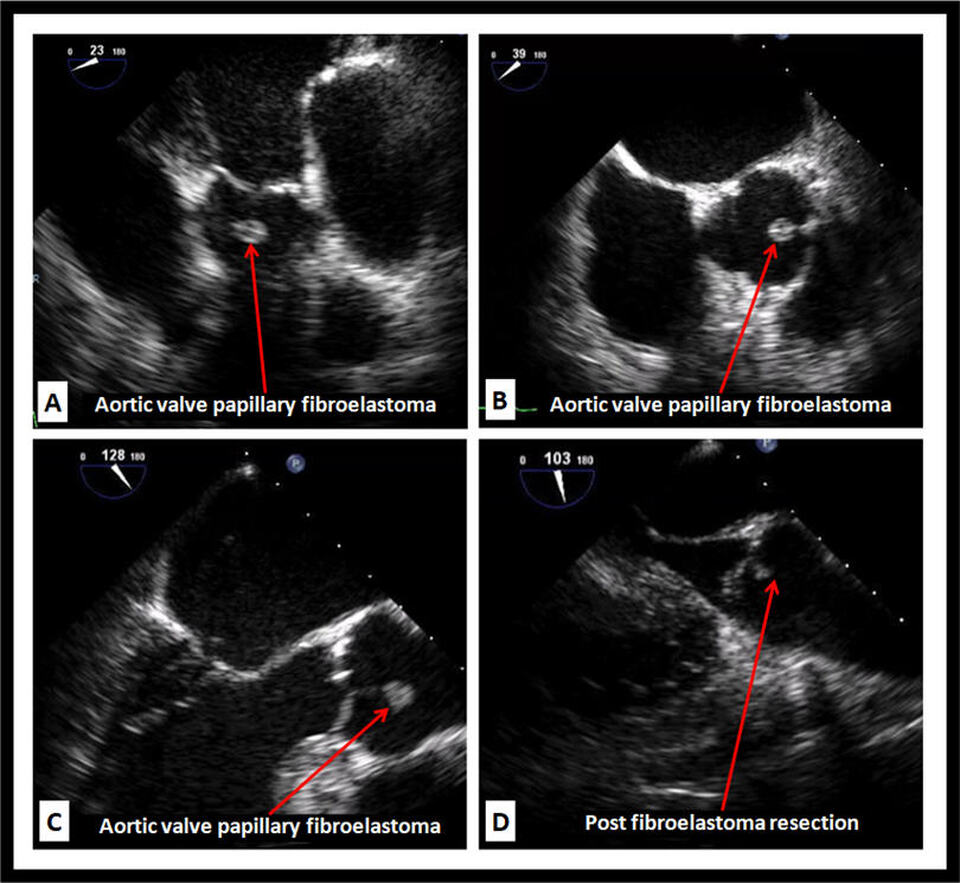
The transesophageal echocardiographic images demonstrate a rounded echodensity on the aortic valve in the deep transgastric view (Figure A), the mid-esophageal short-axis view (Figure B) and the mid-esophageal long-axis view (Figure C) in a patient with recurrent angina and elevated cardiac markers in the absence of obstructive coronary artery disease. Surgical resection of the mass as shown in the mid-esophageal long-axis view (Figure D) resulted in resolution of the symptoms. Pathology revealed papillary fibroelastoma of the aortic valve.
Discussion
Papillary fibroelastomas are among the most common primary cardiac tumors, second only to myxomas [1]. Historically, these tumors were only found upon autopsy and thought to be benign, however, approximately one third of these tumors are diagnosed after an embolic event [2]. Just over half the patients that are diagnosed with these tumors are male, with the average age of diagnosis being 60 years [3]. Approximately 30% of fibroelastomas are diagnosed incidentally and do not cause any symptoms, however, symptoms are typically secondary to embolization with the most common presentation being stroke or transient ischemic attack [4]. Other common presentations include angina [5], myocardial infarction [6], sudden cardiac death [7], heart failure, syncope [8], pulmonary embolism [9] and multiorgan symptoms [10].
Approximately 65% of papillary fibroelastomas affect the left side of the heart and over 80% are located on heart valves. Approximately 36% are found on the aortic valve, 29% on the mitral valve, 11% on the tricuspid valve, and 7% on the pulmonic valve. Most papillary fibroelastomas have a pedunculated shape and are mobile in nature, ranging between 2 mm and 70 mm, and often prolapsing with contractile motion of the heart [11]. Etiology of these tumors is thought to be from hemodynamic trauma secondary to turbulent blood flow in the heart which can cause endothelial damage that leads to formation of a fibroelastoma [12].
Papillary fibroelastomas are typically diagnosed on transthoracic [13] and transesophageal [14] echocardiograms. Transthoracic echocardiography has a sensitivity of 89% and specificity of 88% if the mass is > 2mm in size. Three dimensional imaging such as cardiac CT [15] and cardiac MRI [16] may be beneficial in characterizing the tissue of these masses, however, there is poor temporal resolution making it difficult to assess rapidly moving structures. Multimodality imaging is often helpful in better characterization of these tumors [17].
Surgical removal is recommended for all symptomatic patients due to risk of embolization and increased mortality [18]. Asymptomatic
patients may be routinely monitored [19, 20, 21], but surgery is recommended for any tumor that is large in size or becomes mobile [22]. According to a study performed by Mayo Clinic [23] the stroke risk in surgically managed patients was 2% at one year and 8% at five years. In the conservatively managed group the stroke risk was 6% at one year and 13% at five years. The mechanism by which these tumors cause embolization is thought to be due to either tumor fragments or thrombi connected to the tumor, suggesting a role for anticoagulation in patients not eligible for or awaiting surgery [24].
Conclusion
Papillary fibroelastomas are among the most common primary cardiac tumors and typically are asymptomatic and diagnosed as an incidental finding with no consensus on optimal management [25]. Despite their often small size, they carry a serious embolic potential [26]. Surgery should be considered in anyone diagnosed with papillary fibroelastoma due to the risk for future or worsening embolic events. Further investigation is needed to assess for benefit of anticoagulation in this patient population.
References
Authors:
Alexis Parks, D.O.
Internal Medicine Resident
University of South Alabama
Mobile, AL
Rajasekhar Mulyala, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Nupur Shah, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Nikky Bardia, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Usman Sarwar, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Maulikkumar Patel, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
G. Mustafa Awan, M.D.
Associate Professor of Cardiology
University of South Alabama
Mobile, AL
Christopher Malozzi, D.O.
Associate Professor of Cardiology
University of South Alabama
Mobile, AL
Bassam Omar, M.D., Ph.D.
Professor of Cardiology
University of South Alabama
Mobile, AL
The transesophageal echocardiographic images demonstrate a rounded echodensity on the aortic valve in the deep transgastric view (Figure A), the mid-esophageal short-axis view (Figure B) and the mid-esophageal long-axis view (Figure C) in a patient with recurrent angina and elevated cardiac markers in the absence of obstructive coronary artery disease. Surgical resection of the mass as shown in the mid-esophageal long-axis view (Figure D) resulted in resolution of the symptoms. Pathology revealed papillary fibroelastoma of the aortic valve.
Discussion
Papillary fibroelastomas are among the most common primary cardiac tumors, second only to myxomas [1]. Historically, these tumors were only found upon autopsy and thought to be benign, however, approximately one third of these tumors are diagnosed after an embolic event [2]. Just over half the patients that are diagnosed with these tumors are male, with the average age of diagnosis being 60 years [3]. Approximately 30% of fibroelastomas are diagnosed incidentally and do not cause any symptoms, however, symptoms are typically secondary to embolization with the most common presentation being stroke or transient ischemic attack [4]. Other common presentations include angina [5], myocardial infarction [6], sudden cardiac death [7], heart failure, syncope [8], pulmonary embolism [9] and multiorgan symptoms [10].
Approximately 65% of papillary fibroelastomas affect the left side of the heart and over 80% are located on heart valves. Approximately 36% are found on the aortic valve, 29% on the mitral valve, 11% on the tricuspid valve, and 7% on the pulmonic valve. Most papillary fibroelastomas have a pedunculated shape and are mobile in nature, ranging between 2 mm and 70 mm, and often prolapsing with contractile motion of the heart [11]. Etiology of these tumors is thought to be from hemodynamic trauma secondary to turbulent blood flow in the heart which can cause endothelial damage that leads to formation of a fibroelastoma [12].
Papillary fibroelastomas are typically diagnosed on transthoracic [13] and transesophageal [14] echocardiograms. Transthoracic echocardiography has a sensitivity of 89% and specificity of 88% if the mass is > 2mm in size. Three dimensional imaging such as cardiac CT [15] and cardiac MRI [16] may be beneficial in characterizing the tissue of these masses, however, there is poor temporal resolution making it difficult to assess rapidly moving structures. Multimodality imaging is often helpful in better characterization of these tumors [17].
Surgical removal is recommended for all symptomatic patients due to risk of embolization and increased mortality [18]. Asymptomatic
patients may be routinely monitored [19, 20, 21], but surgery is recommended for any tumor that is large in size or becomes mobile [22]. According to a study performed by Mayo Clinic [23] the stroke risk in surgically managed patients was 2% at one year and 8% at five years. In the conservatively managed group the stroke risk was 6% at one year and 13% at five years. The mechanism by which these tumors cause embolization is thought to be due to either tumor fragments or thrombi connected to the tumor, suggesting a role for anticoagulation in patients not eligible for or awaiting surgery [24].
Conclusion
Papillary fibroelastomas are among the most common primary cardiac tumors and typically are asymptomatic and diagnosed as an incidental finding with no consensus on optimal management [25]. Despite their often small size, they carry a serious embolic potential [26]. Surgery should be considered in anyone diagnosed with papillary fibroelastoma due to the risk for future or worsening embolic events. Further investigation is needed to assess for benefit of anticoagulation in this patient population.
References
- Devanabanda AR, Lee LS. Papillary Fibroelastoma. 2021 Aug 11. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–.
- Brown RD Jr, Khandheria BK, Edwards WD. Cardiac papillary fibroelastoma: a treatable cause of transient ischemic attack and ischemic stroke detected by transesophageal echocardiography. Mayo Clin Proc. 1995 Sep;70(9):863-8.
- Gowda RM, Khan IA, Nair CK, et al. Cardiac papillary fibroelastoma: a comprehensive analysis of 725 cases. Am Heart J. 2003 Sep;146(3):404-10.
- Esteban-Lucía L, De la Fuente Batista S, Kallmeyer Mayor AM, Cortés et al. Cardioembolic Stroke Secondary to an Aortic Valve Fibroelastoma: An Increasingly Recognized Rare Cause of Stroke. Stroke. 2021 Apr;52(4):e111-e114.
- Giambruno V, Karangelis D, Cucchietti C. Aortic Valve Papillary Fibroelastoma: An Insidious and Unusual Cause of Angina. J Cardiothorac Vasc Anesth. 2015 Oct;29(5):e61-3.
- Tang Z, Liu M, Huang H. A rare case of acute myocardial infarction related to mobile papillary fibroelastoma of the aortic valve. Echocardiography. 2021 Oct;38(10):1828-1832.
- Zull DN, Diamond M, Beringer D. Angina and sudden death resulting from papillary fibroelastoma of the aortic valve. Ann Emerg Med. 1985 May;14(5):470-3.
- Maestroni A, Zecca B, Triggiani M. Cardiac papillary fibroelastoma presenting with acute coronary syndrome and syncope. Acta Cardiol. 2006 Jun;61(3):363-5.
- Shah RA, Kalidoss L, Mohanraj A, et al. Papillary fibroelastoma of tricuspid valve presenting as pulmonary embolism. Asian Cardiovasc Thorac Ann. 2015 Sep;23(7):858-60.
- Kaplan JG, Kanwal A, Bahoora J, et al. Papillary fibroelastoma presenting with multi-organ symptoms. J Community Hosp Intern Med Perspect. 2020 Oct 29;10(6):597-599.
- Mignogna C, Amorosi A, Mastroroberto P. Sea Anemone Tumor: Macroscopic Diagnosis of Cardiac Papillary Fibroelastoma. Int J Surg Pathol. 2019 Apr;27(2):185-186.
- Sun JP, Asher CR, Yang XS, et al. Clinical and echocardiographic characteristics of papillary fibroelastomas: a retrospective and prospective study in 162 patients. Circulation. 2001 Jun 5;103(22):2687-93.
- Rana Y, Tummala R, Engstrom K, et al. Discovery of Tricuspid Fibroelastoma on Echocardiography. Cureus. 2021 Aug 22;13(8):e17359.
- Cook AG, Viswanath O, D'Mello J. Papillary Fibroelastoma Found With Transesophageal Echocardiography After a Normal Transthoracic Echocardiography. Semin Cardiothorac Vasc Anesth. 2017 Sep;21(3):217-220.
- Kim AY, Kim JS, Yoon Y, et al. Multidetector computed tomography findings of a papillary fibroelastoma of the aortic valve: a case report. J Korean Med Sci. 2010 May;25(5):809-12.
- van der Meulen TA, Budde RP, Randjgari A, et al. Multimodality imaging of a papillary fibroelastoma of the mitral valve. Eur J Cardiothorac Surg. 2012 Oct;42(4):747-8.
- Hoey ET, Shahid M, Ganeshan A, et al. MRI assessment of cardiac tumours: part 1, multiparametric imaging protocols and spectrum of appearances of histologically benign lesions. Quant Imaging Med Surg. 2014 Dec;4(6):478-88.
- Ngaage DL, Mullany CJ, Daly RC, et al. Surgical treatment of cardiac papillary fibroelastoma: a single center experience with eighty-eight patients. Ann Thorac Surg. 2005 Nov;80(5):1712-8.
- Grande AM, Castiglione N, Iervolino A, Nappi F, et al. Nonsurgical Management of a Papillary Fibroelastoma of the Aortic Valve. Case Rep Cardiol. 2021 Jul 6;2021:4160793.
- Seol SH, Kim DS, Han YC, et al. Nonsurgical management of a tricuspid valvular pedunculated papillary fibroelastoma. Cardiovasc Ultrasound. 2009 Sep 4;7:44.
- Bauch T, Htun W. Medical Management of Papillary Fibroelastoma is Associated With Low Risk of Embolization in Selected Cases. Circulation. 2015;132:A18173
- Grinda JM, Couetil JP, Chauvaud S, et al. Cardiac valve papillary fibroelastoma: surgical excision for revealed or potential embolization. J Thorac Cardiovasc Surg. 1999 Jan;117(1):106-10.
- Tamin SS, Maleszewski JJ, Scott CG, et al. Prognostic and Bioepidemiologic Implications of Papillary Fibroelastomas. J Am Coll Cardiol. 2015 Jun 9;65(22):2420-9.
- Toyama M, Abe T, Nakayama M, et al. [Effective Anticoagulation Therapy Prior to Surgical Excision of an Aortic Valve Papillary Fibroelastoma Diagnosed after a Transient Cerebral Ischemic Attack;Report of a Case]. Kyobu Geka. 2017 Apr;70(4):317-319. Japanese.
- Chhabra L, Joshi S, Chaubey VK, et al. Incidental cardiac papillary fibroelastoma: a management dilemma. BMJ Case Rep. 2013 Aug 7;2013:bcr2013200133.
- Sousa-Uva M, Cardim N. Cardiac papillary fibroelastoma: So small and yet so dangerous. Rev Port Cardiol (Engl Ed). 2018 Dec;37(12):987-989. English, Portuguese.
Authors:
Alexis Parks, D.O.
Internal Medicine Resident
University of South Alabama
Mobile, AL
Rajasekhar Mulyala, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Nupur Shah, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Nikky Bardia, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Usman Sarwar, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Maulikkumar Patel, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
G. Mustafa Awan, M.D.
Associate Professor of Cardiology
University of South Alabama
Mobile, AL
Christopher Malozzi, D.O.
Associate Professor of Cardiology
University of South Alabama
Mobile, AL
Bassam Omar, M.D., Ph.D.
Professor of Cardiology
University of South Alabama
Mobile, AL