
August 2020 Issue
ISSN 2689-291X
ISSN 2689-291X
ACAOS Double Whammy..
Single Coronary & Malignant RCA Course!
Description
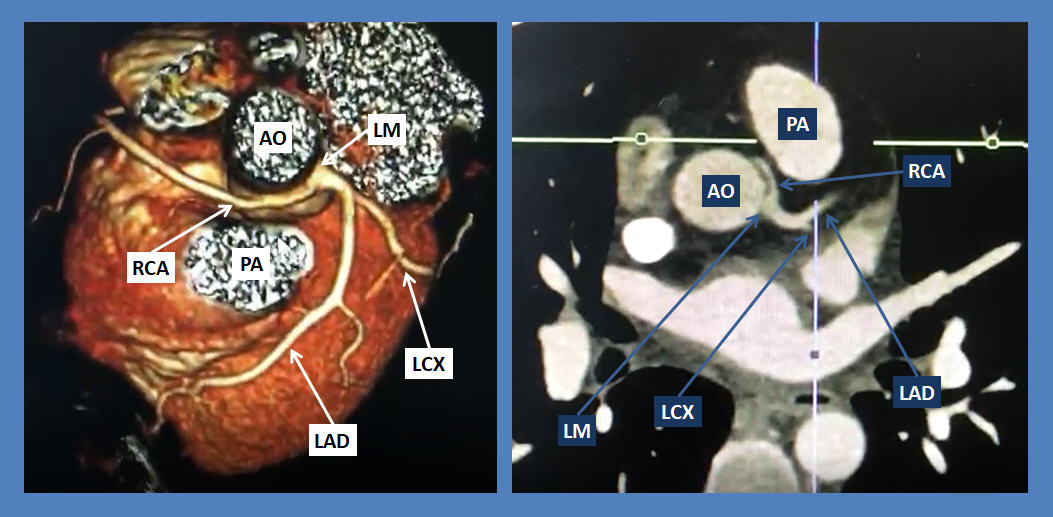
The above volume rendered and maximum intensity projection (MIP) CT angiography images and the accompanying video clips show an anomalous origin of the right coronary artery (RCA) from the opposite sinus of Valsalva (ACAOS), a rare congenital anomaly.
The RCA originates from the ostial left main (LM) coronary artery proximal to the bifurcation of the left anterior descending (LAD) and left circumflex (LCX) coronary arteries, resulting in a rare “single coronary artery” anomaly configuration. The course of the RCA is between the major aortic (AO) and pulmonary (PA) trunks, a malignant course which may predispose to ischemia, arrhythmia and sudden cardiac death.
Discussion:
Coronary anomalous origin is rare with a prevalence of 0.17 % in one autopsy report [1]. The prevalence can be up to 1.2 % with coronary angiography [2] and 2.3% on multidetector coronary tomography (MDCT) coronary angiography [3]. Nearly one fifth of cases can be associated with malignant outcomes [4].
Many cases of congenital coronary anomalies are sporadic and are discovered incidentally; however a familial tendency has been reported in some cases [5]. Association with other congenital heart disease such as Holt Oram has also been reported [6] and hypertrophic cardiomyopathy [7].
Assessment of congenital coronary anomalies often requires multimodality imaging and angiography approach aiming at identifying the structural abnormality and its functional significance [8]. Management of coronary artery disease anomalies will depend on the results of such studies and may requires surgical correction in malignant cases [9].
ACAOS has been reported with a prevalence of 0.7% in the population [10], with more prevalence of an anomalous origin of the RCA from the left coronary sinus. Nearly half of the ACAOS cases showed a malignant course. Cases with a separate ostium of the RCA from the left coronary sinus have been reported [11], including in the setting of a positive stress test [12] with the RCA coursing between the major pulmonary and aortic trunks, predisposing to coronary compression and malignant outcomes. Familial clustering of ACAOS has also been reported [13]. The management of ACAOS depends on the particular anatomic and physiologic aspects of the anomaly and can vary from medical to surgical management [14].
A rarer variant of ACAOS is the origin of the RCA from the LM, as in the images presented earlier. Earlier reports of such rare anomaly have shown successful surgical treatment to relieve angina [15]. Another case report of a rare origin of the RCA from the middle of the LAD was also treated surgically [16]. These cases of a “single coronary artery” which can also arise from the right coronary sinus [17] present both a diagnostic and management dilemma and often would require surgical intervention [18].
References:
Authors:
Muhammad Rafique, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Siva Chiranjeevi, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Nilarun Chowdhuri, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Amod Amritphale, M.D.
Assistant Professor of Cardiology
University of South Alabama
Mobile, AL
G. Mustafa Awan, M.D.
Associate Professor of Cardiology
University of South Alabama
Mobile, AL
Christopher Malozzi, D.O.
Assistant Professor of Cardiology
University of South Alabama
Mobile, AL
Farnoosh Rahimi, M.D.
Assistant Professor of Cardiology
University of South Alabama
Mobile, AL
Bassam Omar, M.D., Ph.D.
Professor of Cardiology
University of South Alabama
Mobile, AL
Keerthana Karumbaiah, M.D.
Staff Cardiologist
Shannon Clinic
San Angelo, TX
The above volume rendered and maximum intensity projection (MIP) CT angiography images and the accompanying video clips show an anomalous origin of the right coronary artery (RCA) from the opposite sinus of Valsalva (ACAOS), a rare congenital anomaly.
The RCA originates from the ostial left main (LM) coronary artery proximal to the bifurcation of the left anterior descending (LAD) and left circumflex (LCX) coronary arteries, resulting in a rare “single coronary artery” anomaly configuration. The course of the RCA is between the major aortic (AO) and pulmonary (PA) trunks, a malignant course which may predispose to ischemia, arrhythmia and sudden cardiac death.
Discussion:
Coronary anomalous origin is rare with a prevalence of 0.17 % in one autopsy report [1]. The prevalence can be up to 1.2 % with coronary angiography [2] and 2.3% on multidetector coronary tomography (MDCT) coronary angiography [3]. Nearly one fifth of cases can be associated with malignant outcomes [4].
Many cases of congenital coronary anomalies are sporadic and are discovered incidentally; however a familial tendency has been reported in some cases [5]. Association with other congenital heart disease such as Holt Oram has also been reported [6] and hypertrophic cardiomyopathy [7].
Assessment of congenital coronary anomalies often requires multimodality imaging and angiography approach aiming at identifying the structural abnormality and its functional significance [8]. Management of coronary artery disease anomalies will depend on the results of such studies and may requires surgical correction in malignant cases [9].
ACAOS has been reported with a prevalence of 0.7% in the population [10], with more prevalence of an anomalous origin of the RCA from the left coronary sinus. Nearly half of the ACAOS cases showed a malignant course. Cases with a separate ostium of the RCA from the left coronary sinus have been reported [11], including in the setting of a positive stress test [12] with the RCA coursing between the major pulmonary and aortic trunks, predisposing to coronary compression and malignant outcomes. Familial clustering of ACAOS has also been reported [13]. The management of ACAOS depends on the particular anatomic and physiologic aspects of the anomaly and can vary from medical to surgical management [14].
A rarer variant of ACAOS is the origin of the RCA from the LM, as in the images presented earlier. Earlier reports of such rare anomaly have shown successful surgical treatment to relieve angina [15]. Another case report of a rare origin of the RCA from the middle of the LAD was also treated surgically [16]. These cases of a “single coronary artery” which can also arise from the right coronary sinus [17] present both a diagnostic and management dilemma and often would require surgical intervention [18].
References:
- Alexander RW, Griffith GC. Anomalies of the coronary arteries and their clinical significance. Circulation. 1956;14:800–5.
- Engel HJ, Torres C, Page HL. Major variations in anatomical origin of the coronary arteries: angiographic observations in 4250 patients without congenital heart disease. Cathet Cardiovasc Diagn. 1975;1:157–69.
- Graidis C, Dimitriadis D, Karasavvidis V, et al. Prevalence and characteristics of coronary artery anomalies in an adult population undergoing multidetector-row computed tomography for the evaluation of coronary artery disease. BMC Cardiovasc Disord. 2015;15:112. Published 2015 Oct 2.
- Datta J, White CS, Gilkeson RC, Meyer CA, Kansal S, Jani ML, et al. Anomalous coronary arteries in adults: Depiction at multidetector row CT angiography. Radiology. 2005;235(3):812–8. Epub 2005 Apr 15.
- Laureti JM, Singh K, Blankenship J. Anomalous coronary arteries: a familial clustering. Clin Cardiol. 2005;28(10):488-490.
- Aung TT, Roberto ES, Wase A. Absent Left Main Coronary Artery and Separate Ostia of Left Coronary System in a Patient with Holt-Oram Syndrome and Sinus Node Dysfunction. Am J Case Rep. 2016 Feb 17;17:93-6.
- Liddy S, Roy AK, McCreery C. Double trouble: hypertrophic cardiomyopathy coexistent with malignant anomalous right coronary artery. BMJ Case Rep. 2014 Mar 28;2014:bcr2013203344.
- Gräni C, Kaufmann PA, Windecker S, Buechel RR. Diagnosis and Management of Anomalous Coronary Arteries with a Malignant Course. Interv Cardiol. 2019;14(2):83-88. Published 2019 May 21.
- King NM, Tian DD, Munkholm-Larsen S, Buttar SN, Chow V, Yan T. The Aberrant Coronary Artery - The Management Approach. Heart Lung Circ. 2018;27(6):702-707.
- Nezarat N, Luo Y, Darabian S, et al. Prevalence and long term follow-up of anomalous coronary arteries originating from the opposite sinus (ACAOS). J Am Coll Cardiol. 2015 March; (5)10S:A500.
- Kolakalapudi P, Sachdev S, Omar B. Anomalous Coronary! Is It Time To Panic! Cardiofel Newslet 2019 April; 2(4): 13-14.
- Setianto BY, Hartopo AB, Gharini PP, Taufiq N. Anomalous Origination of Right Coronary Artery from Left Sinus in Asymptomatic Young Male Presenting with Positive Ischemic Response on Treadmill Test. Case Rep Cardiol. 2016;2016:7652869.
- Youniss MA, Ghoshhajra B, Bernard S, et al. Familial Anomalous Origin of Right Coronary Artery from the Left Coronary Sinus. Am J Cardiol. 2018;122(10):1800-1802.
- Mursleen A, Hartlage G, Patel A, Harrison EE, Morales CA. Diagnosis Using CCTA and Management of Anomalous Right Coronary Artery from the Opposite Sinus. Case Rep Cardiol. 2016;2016:7685360.
- Lopushinsky S, Mullen J, Bentley M. Anomalous Right Coronary Artery Originating From the Left Main Coronary Artery. Ann Thorac Surg 2001;71:357–8.
- Tokmakoglu H, Bozoglan O, Ozdemir L. Right coronary artery originating from left anterior descending artery: a case report. J Cardiothorac Surg. 2010 Jun 8;5:49.
- Ghaffari S, Pourafkari L, Nader ND. Single Coronary Artery: Pete Maravich Anomaly Revisited. Am J Med Sci. 2016;351(4):435-436.
- Guria RT, Gupta U. Report on a rare single coronary artery anomaly: Need for comprehensive investigations. J Family Med Prim Care. 2017 Apr-Jun;6(2):424-426.
Authors:
Muhammad Rafique, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Siva Chiranjeevi, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Nilarun Chowdhuri, M.D.
Cardiology Fellow
University of South Alabama
Mobile, AL
Amod Amritphale, M.D.
Assistant Professor of Cardiology
University of South Alabama
Mobile, AL
G. Mustafa Awan, M.D.
Associate Professor of Cardiology
University of South Alabama
Mobile, AL
Christopher Malozzi, D.O.
Assistant Professor of Cardiology
University of South Alabama
Mobile, AL
Farnoosh Rahimi, M.D.
Assistant Professor of Cardiology
University of South Alabama
Mobile, AL
Bassam Omar, M.D., Ph.D.
Professor of Cardiology
University of South Alabama
Mobile, AL
Keerthana Karumbaiah, M.D.
Staff Cardiologist
Shannon Clinic
San Angelo, TX