
January 2021 Issue
ISSN 2689-291X
ISSN 2689-291X
McConnell’s Sign..
RV Strain in Acute Pulmonary Embolism!
Description
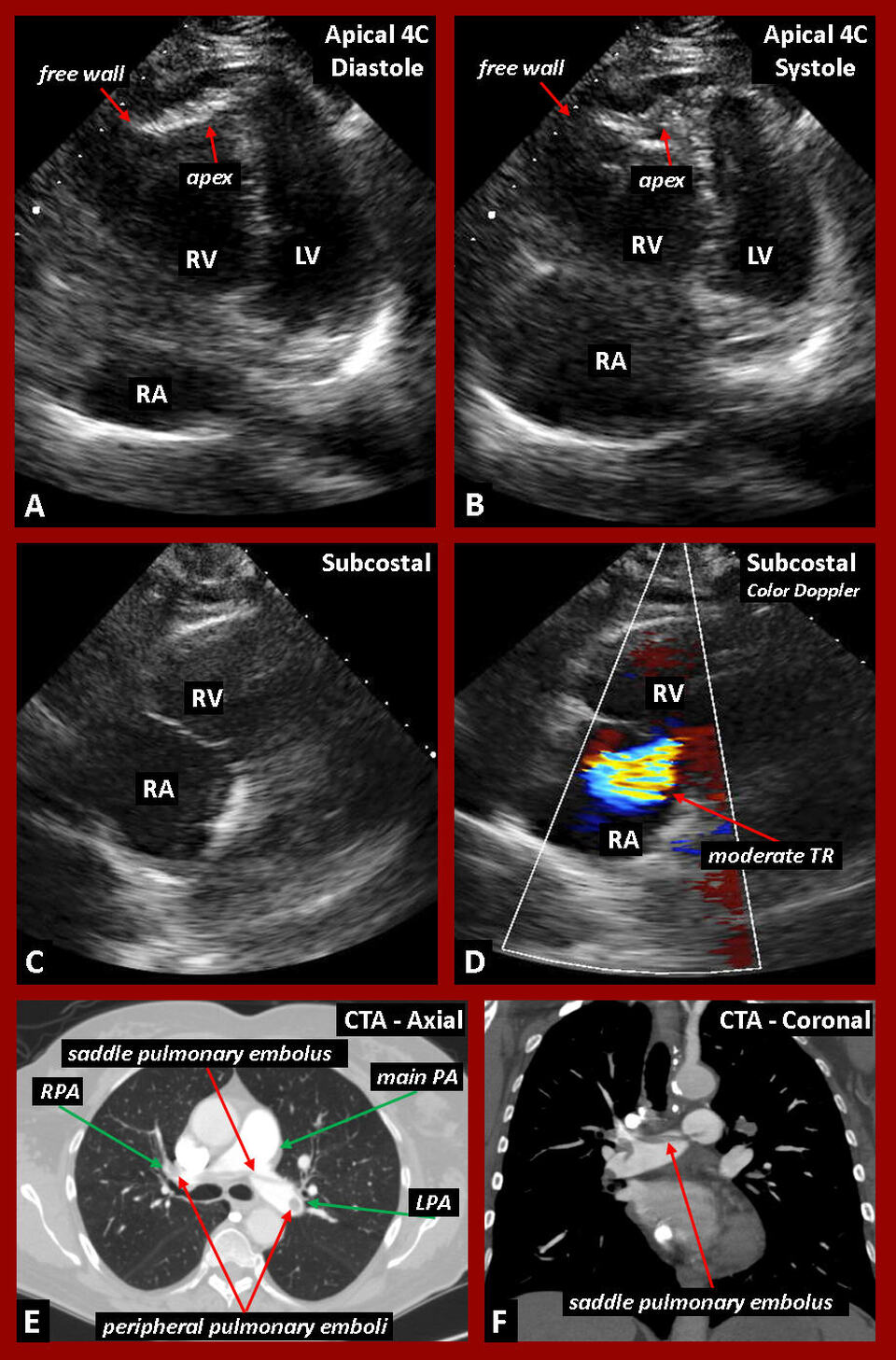
The figure above shows 2-D echocardiographic images (A-D) and computed tomographic angiography (CTA) images (E & F) associated with massive pulmonary embolism. In Figure A, apical 4-chamber (4C) image in diastole reveals a massively dilated right ventricle (RV) and right atrium (RA) compared to a small, relatively underfilled left ventricle (LV). In Figure B, apical 4C image in systole reveals indentation of the RV apex indicative of normal to hyperdynamic function, while there is near akinesis of the RV free wall; this differential regional wall motion abnormality is a sign of acute RV strain consistent with McConnell’s sign. In Figure C, 2-D subcostal image reveals dilatation of the right heart chambers and the tricuspid valve annulus; which causes moderate tricuspid regurgitation (TR) as seen in Figure D. The CT angiographic images in the Axial plane (Figure E) and the Coronal plane (Figure F) reveal a massive saddle pulmonary embolus, with peripheral emboli, as the cause of the observed RV strain and McConnell’s sign.
Discussion
Pulmonary embolism is a fatal disease which requires prompt diagnosis and treatment [1]. The presence and extent of right ventricular strain correlate with the severity of the pulmonary embolism and portend poorer prognosis; this should therefore be evaluated early to determine the need for rapid intervention [2].
McConnell’s sign is a well-described echocardiographic finding associated with acute pulmonary embolism. It is defined as regional right ventricular dysfunction, with akinesis of the mid free wall but normal motion at the apex [3]. McConnell’s sign identified on echocardiogram is a highly specific, although not very sensitive finding in acute pulmonary embolism. A meta-analysis of the use of transthoracic echocardiography in diagnosing pulmonary embolism found it to have a sensitivity of 22% and specificity of 97% [4]. Rarely, McConnell’s sign may be seen in alternative etiologies including malignancy [5]. Echocardiography can yield important prognostic information for high-risk patients who cannot otherwise be evaluated with contrasted chest tomography or pulmonary V/Q scan in a timely manner including but not limited to the following: renal dysfunction, pregnancy, allergy to intravenous contrast agents, and body habitus limitations [4].
Management of acute pulmonary embolism varies and often depends on the severity of the presentation [6]. Systemic thrombolytic agents have long been successfully used in the treatment of thromboembolism [7], with interventional and surgical approaches or hybrid techniques employed in severe cases associated with circulatory shock [8]. Echocardiography has evolved as a valuable tool to help in the diagnosis and assess the prognosis of pulmonary embolism, and to guide acute treatment and long term follow-up [9].
References:
Authors:
Ashley Andrews, D.O.
Internal Medicine Resident
University of South Alabama
Mobile, AL
Kaleb Malone, B.S.
Medical Student (MIII)
University of South Alabama
Mobile, AL
Bassam Omar, M.D., Ph.D.
Professor of Cardiology
University of South Alabama
Mobile, AL
The figure above shows 2-D echocardiographic images (A-D) and computed tomographic angiography (CTA) images (E & F) associated with massive pulmonary embolism. In Figure A, apical 4-chamber (4C) image in diastole reveals a massively dilated right ventricle (RV) and right atrium (RA) compared to a small, relatively underfilled left ventricle (LV). In Figure B, apical 4C image in systole reveals indentation of the RV apex indicative of normal to hyperdynamic function, while there is near akinesis of the RV free wall; this differential regional wall motion abnormality is a sign of acute RV strain consistent with McConnell’s sign. In Figure C, 2-D subcostal image reveals dilatation of the right heart chambers and the tricuspid valve annulus; which causes moderate tricuspid regurgitation (TR) as seen in Figure D. The CT angiographic images in the Axial plane (Figure E) and the Coronal plane (Figure F) reveal a massive saddle pulmonary embolus, with peripheral emboli, as the cause of the observed RV strain and McConnell’s sign.
Discussion
Pulmonary embolism is a fatal disease which requires prompt diagnosis and treatment [1]. The presence and extent of right ventricular strain correlate with the severity of the pulmonary embolism and portend poorer prognosis; this should therefore be evaluated early to determine the need for rapid intervention [2].
McConnell’s sign is a well-described echocardiographic finding associated with acute pulmonary embolism. It is defined as regional right ventricular dysfunction, with akinesis of the mid free wall but normal motion at the apex [3]. McConnell’s sign identified on echocardiogram is a highly specific, although not very sensitive finding in acute pulmonary embolism. A meta-analysis of the use of transthoracic echocardiography in diagnosing pulmonary embolism found it to have a sensitivity of 22% and specificity of 97% [4]. Rarely, McConnell’s sign may be seen in alternative etiologies including malignancy [5]. Echocardiography can yield important prognostic information for high-risk patients who cannot otherwise be evaluated with contrasted chest tomography or pulmonary V/Q scan in a timely manner including but not limited to the following: renal dysfunction, pregnancy, allergy to intravenous contrast agents, and body habitus limitations [4].
Management of acute pulmonary embolism varies and often depends on the severity of the presentation [6]. Systemic thrombolytic agents have long been successfully used in the treatment of thromboembolism [7], with interventional and surgical approaches or hybrid techniques employed in severe cases associated with circulatory shock [8]. Echocardiography has evolved as a valuable tool to help in the diagnosis and assess the prognosis of pulmonary embolism, and to guide acute treatment and long term follow-up [9].
References:
- Olin JW. Pulmonary embolism. Rev Cardiovasc Med. 2002;3 Suppl 2:S68-75.
- Lee K, Kwon O, Lee EJ, Sin MJ, Lee JS, Lee S, Kang DH, Song JK, Song JM. Prognostic value of echocardiographic parameters for right ventricular function in patients with acute non-massive pulmonary embolism. Heart Vessels. 2019 Jul;34(7):1187-1195.
- Oh SB, Bang SJ, Kim MJ. McConnell’s sign; a distinctive echocardiographic finding for diagnosing acute pulmonary embolism in emergency department. Crit Ultrasound J. 2015;7(Suppl 1):A20. Published 2015 Mar 9.
- Kansara T, Quesada F, Park H, et al. (November 26, 2019) McConnell’s Sign Still Holds Its Value: A Lesson Learned from Two Cases. Cureus 11(11): e6240.
- Antoine S, Oye M. McConnell’s sign in invasive small cell lung cancer. Chest, Volume 158, Issue 4, Supplement. Published 2020.
- Hepburn-Brown M, Darvall J, Hammerschlag G. Acute pulmonary embolism: a concise review of diagnosis and management. Intern Med J. 2019 Jan;49(1):15-27.
- Konstantinides SV, Barco S. Systemic Thrombolytic Therapy for Acute Pulmonary Embolism: Who Is a Candidate? Semin Respir Crit Care Med. 2017 Feb;38(1):56-65.
- Dudzinski DM, Giri J, Rosenfield K. Interventional Treatment of Pulmonary Embolism. Circ Cardiovasc Interv. 2017 Feb;10(2):e004345.
- Dutta T, Frishman WH, Aronow WS. Echocardiography in the Evaluation of Pulmonary Embolism. Cardiol Rev. 2017 Nov/Dec;25(6):309-314.
Authors:
Ashley Andrews, D.O.
Internal Medicine Resident
University of South Alabama
Mobile, AL
Kaleb Malone, B.S.
Medical Student (MIII)
University of South Alabama
Mobile, AL
Bassam Omar, M.D., Ph.D.
Professor of Cardiology
University of South Alabama
Mobile, AL