
March 2022 Issue
ISSN 2689-291X
ISSN 2689-291X
Left Main to Pulmonary Artery Coronary Fistula:
Surgical Closure!
Description
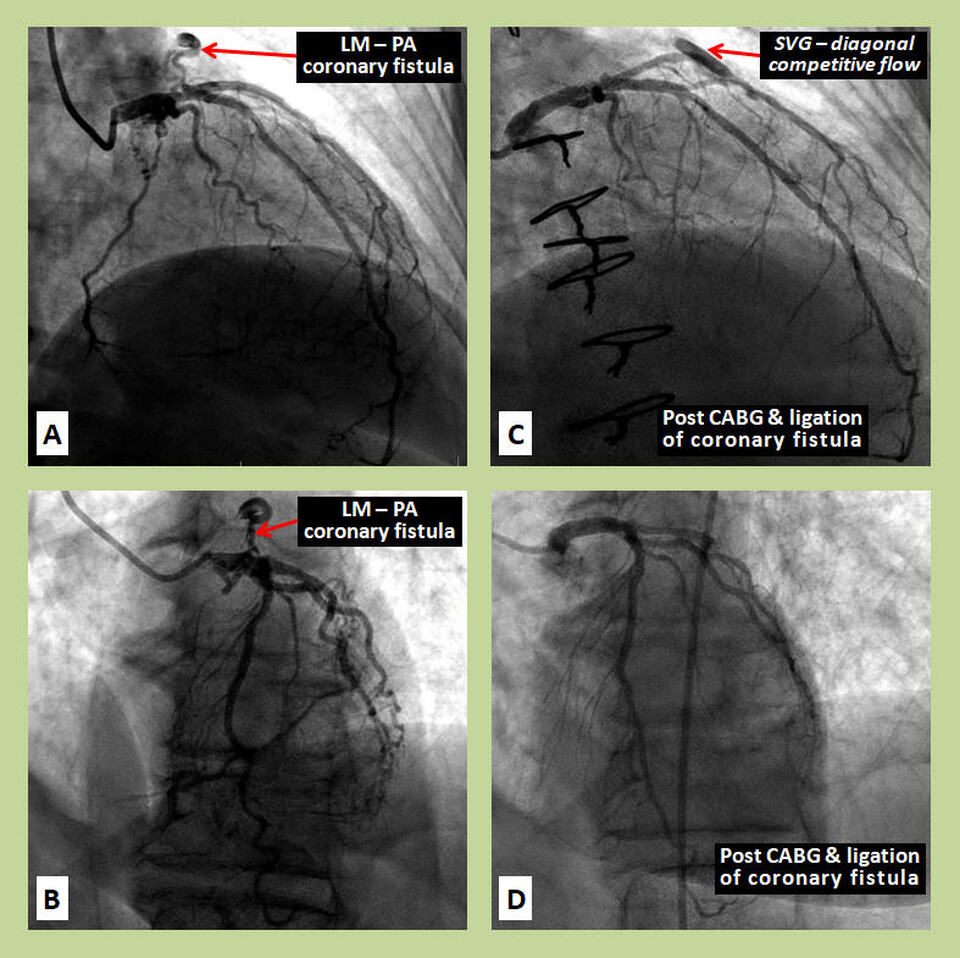
The coronary angiographic images in the right anterior oblique (RAO) cranial (Figures A) and left anterior oblique (LAO) cranial (Figure B) demonstrate a large coronary fistula connecting the left main coronary artery to the main pulmonary artery (LM – PA coronary fistula). Significant multivessel coronary artery disease, in the setting of angina and demonstrated ischemia on stress nuclear imaging, necessitated coronary artery bypass grafting (CABG) during which the fistula was ligated. The post-CABG angiogram (Figure C) demonstrated absence of the fistula; competitive flow into the saphenous vein graft (SVG) to the diagonal branch can also been seen. The LAO caudal view (Figure D) confirms the disappearance of the fistula.
Discussion
Coronary artery fistula (CAF) is rare cardiac defect where a coronary artery abnormally connects to another blood vessel or heart chamber and bypasses the myocardial capillary bed. The reported incidence of CAF in one study was 0.9% of all coronary computed tomographic angiography (CTA) images done [1]. CAF can be congenital [2] or may be acquired following cardiac surgery [3], coronary artery bypass grafting [4], valve replacement [5], repeated cardiac biopsies [6] and nonpenetrating chest trauma [7]. CAF are subdivided based on the structure into which the abnormal coronary connection drains: if CAF drains into a heart chamber it is referred to as coronary-cameral fistula while CAF which drains into another blood vessel it is referred to as coronary-arteriovenous (AV) fistula [8].
Pathophysiology of CAF depends on its origin, insertion site, and amount of blood it shunts. CAF's most commonly arise from right coronary artery and most commonly connect to right ventricle [9, 10]. CAF has a heterogeneous presentation [11] and may be asymptomatic; symptoms, however, can develop after two decades of life. Symptomatic CAF may present with fatigue, dyspnea, orthopnea [12], arrhythmias [13], myocardial infarction [14], and rarely pericardial effusions [15] and cardiac tamponade [16]. Other serious reported symptoms include angina due to coronary steal [17], syncope [18], and sudden death [19].
Many CAFs are found incidentally on CTAs obtained for unrelated reasons [20]. Other tools of evaluation include transthoracic echocardiography [21] which may be able to visualize a hemodynamically significant CAF, and transesophageal echocardiography [22]. Studies such as electrocardiograms and chest x-ray are not very helpful in the diagnosis. Coronary angiography and cardiac catheterization are the gold standard for the evaluation and diagnosis of CAFs, but often multimodality imaging may be needed for optimal characterization [23].
The main indications for closure of CAF are hemodynamically significant shunting causing heart failure, myocardial ischemia, or large left-to-right shunting [24]. CAF closure can be achieved through percutaneous techniques such as embolization or open heart surgery. Surgical intervention involves internal closure of coronary fistula and ligation within the aneurysm; this method achieves complete occlusion in more than 95% of cases and can be performed off pump [25] and by thoracoscopy [26]. Catheter closure of coronary fistula is less invasive than surgical intervention, and the occlusion can be achieved more distally avoiding potential branch vessel occlusion. Embolization may be achieved by balloon [27], coils [28], and micro-coils [29]. Ultimately the method and materials will depend on the morphology of CAF; highly tortuous and large fistulas may warrant surgical intervention [30]. Reassessment with coronary angiography is done post-embolization to evaluate for complete closure of CAF and treatment with antiplatelet agents is warranted.
References
Authors:
Valeria Pierluissi Rivera, M.D.
Internal Medicine Resident
University of South Alabama
Mobile, AL
Bassam Omar, M.D., Ph.D.
Professor of Cardiology
University of South Alabama
Mobile, AL
The coronary angiographic images in the right anterior oblique (RAO) cranial (Figures A) and left anterior oblique (LAO) cranial (Figure B) demonstrate a large coronary fistula connecting the left main coronary artery to the main pulmonary artery (LM – PA coronary fistula). Significant multivessel coronary artery disease, in the setting of angina and demonstrated ischemia on stress nuclear imaging, necessitated coronary artery bypass grafting (CABG) during which the fistula was ligated. The post-CABG angiogram (Figure C) demonstrated absence of the fistula; competitive flow into the saphenous vein graft (SVG) to the diagonal branch can also been seen. The LAO caudal view (Figure D) confirms the disappearance of the fistula.
Discussion
Coronary artery fistula (CAF) is rare cardiac defect where a coronary artery abnormally connects to another blood vessel or heart chamber and bypasses the myocardial capillary bed. The reported incidence of CAF in one study was 0.9% of all coronary computed tomographic angiography (CTA) images done [1]. CAF can be congenital [2] or may be acquired following cardiac surgery [3], coronary artery bypass grafting [4], valve replacement [5], repeated cardiac biopsies [6] and nonpenetrating chest trauma [7]. CAF are subdivided based on the structure into which the abnormal coronary connection drains: if CAF drains into a heart chamber it is referred to as coronary-cameral fistula while CAF which drains into another blood vessel it is referred to as coronary-arteriovenous (AV) fistula [8].
Pathophysiology of CAF depends on its origin, insertion site, and amount of blood it shunts. CAF's most commonly arise from right coronary artery and most commonly connect to right ventricle [9, 10]. CAF has a heterogeneous presentation [11] and may be asymptomatic; symptoms, however, can develop after two decades of life. Symptomatic CAF may present with fatigue, dyspnea, orthopnea [12], arrhythmias [13], myocardial infarction [14], and rarely pericardial effusions [15] and cardiac tamponade [16]. Other serious reported symptoms include angina due to coronary steal [17], syncope [18], and sudden death [19].
Many CAFs are found incidentally on CTAs obtained for unrelated reasons [20]. Other tools of evaluation include transthoracic echocardiography [21] which may be able to visualize a hemodynamically significant CAF, and transesophageal echocardiography [22]. Studies such as electrocardiograms and chest x-ray are not very helpful in the diagnosis. Coronary angiography and cardiac catheterization are the gold standard for the evaluation and diagnosis of CAFs, but often multimodality imaging may be needed for optimal characterization [23].
The main indications for closure of CAF are hemodynamically significant shunting causing heart failure, myocardial ischemia, or large left-to-right shunting [24]. CAF closure can be achieved through percutaneous techniques such as embolization or open heart surgery. Surgical intervention involves internal closure of coronary fistula and ligation within the aneurysm; this method achieves complete occlusion in more than 95% of cases and can be performed off pump [25] and by thoracoscopy [26]. Catheter closure of coronary fistula is less invasive than surgical intervention, and the occlusion can be achieved more distally avoiding potential branch vessel occlusion. Embolization may be achieved by balloon [27], coils [28], and micro-coils [29]. Ultimately the method and materials will depend on the morphology of CAF; highly tortuous and large fistulas may warrant surgical intervention [30]. Reassessment with coronary angiography is done post-embolization to evaluate for complete closure of CAF and treatment with antiplatelet agents is warranted.
References
- Lim JJ, Jung JI, Lee BY, et al. Prevalence and types of coronary artery fistulas detected with coronary CT angiography. AJR Am J Roentgenol. 2014 Sep;203(3):W237-43.
- Geller CM, Dimitrova KR, Hoffman DM, et al. Congenital coronary artery fistulae: a rare cause of heart failure in adults. J Cardiothorac Surg. 2014 May 16;9:87. doi: 10.1186/1749-8090-9-87.
- Chiu SN, Wu MH, Lin MT, et al. Acquired coronary artery fistula after open heart surgery for congenital heart disease. Int J Cardiol. 2005 Aug 18;103(2):187-92.
- Chen K, Scridon T, Chait R. Inadvertent aortocoronary arteriovenous fistula after CABG: Systematic review of case reports. Catheter Cardiovasc Interv. 2021 Jan 1;97(1):E19-E25.
- Sujatha M, Suneel PR, Bineesh RK. Acquired Coronary Cameral Fistula Following Aortic Valve Replacement. J Cardiothorac Vasc Anesth. 2016 Apr;30(2):455-8.
- Rali AS, Sami F, Sauer A, et al. Right Coronary Artery to Coronary Sinus Fistula Post Endomyocardial Biopsy: A Case Report of a Rare Complication. Case Rep Cardiol. 2020 Mar 1;2020:7914737.
- Forker AD, Morgan JR. Acquired coronary artery fistula from nonpenetrating chest injury. JAMA. 1971 Jan 11;215(2):289-91.
- Qureshi SA. Coronary arterial fistulas. Orphanet J Rare Dis. 2006 Dec 21;1:51.
- Rao SS, Agasthi P. Coronary Artery Fistula. 2021 Dec 26. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan–.
- Sachdev S, Tahir H, Nguyen L, et al. Coronary Fistula: The Anomalous Tributary! Cardiofel Newslet 2019 Feb; 2(2): 5-6.
- Zamani H, Meragi M, Arabi Moghadam MY, et al. Clinical presentation of coronary arteriovenous fistula according to age and anatomic orientation. Caspian J Intern Med. 2015 Spring;6(2):108-12.
- Rivera IR, Moises VA, Tebexreni AS, et al. Right coronary artery fistula with congestive heart failure in the neonate. Doppler echocardiographic diagnosis and closure with detachable balloon. Arq Bras Cardiol. 2000 Mar;74(3):243-52.
- Hickman S, Hobson N, Caldwell J, et al. Exercise-induced ventricular arrhythmia in coronary cameral fistula: A manifestation of reperfusion injury. J Arrhythm. 2021 May 6;37(3):698-700.
- Smettei OA, Abazid RM. A rare case of coronary artery fistula presented with acute myocardial infarction. Avicenna J Med. 2015 Apr-Jun;5(2):49-51.
- Ozeki S, Utsunomiya T, Kishi T, et al. Coronary arteriovenous fistula presenting as chronic pericardial effusion. Circ J. 2002 Aug;66(8):779-82.
- Hijikata S, Sakurai K, Maeba S, et al. Cardiac tamponade due to ruptured coronary-pulmonary artery fistula aneurysm: a case report. Eur Heart J Case Rep. 2020 May 3;4(3):1-5.
- Pagni S, Austin EH, Abraham JS. Right coronary artery to superior vena cava fistula presenting with 'steal' phenomenon. Interact Cardiovasc Thorac Surg. 2004 Dec;3(4):573-4.
- Meric M, Yuksel S. Diffuse Coronary Artery Fistula Leading to Syncope and Treated with Transcatheter Coil Occlusion and a Defibrillator: A Case Report. Med Princ Pract. 2019;28(5):493-496.
- Lau G. Sudden death arising from a congenital coronary artery fistula. Forensic Sci Int. 1995 May 22;73(2):125-30.
- Zenooz NA, Habibi R, Mammen L, et al. Coronary artery fistulas: CT findings. Radiographics. 2009 May-Jun;29(3):781-9.
- Acitelli A, Bencivenga S, Giannico MB, et al. Coronary Artery Fistula Diagnosed by Echocardiography during NSTEMI: Case Report and Review of Literature. Case Rep Cardiol. 2019 Aug 14;2019:5956806.
- Prewitt KC, Smolin MR, Coster TS, et al. Coronary artery fistula diagnosed by transesophageal echocardiography. Chest. 1994 Mar;105(3):959-61.
- Sousa C, Martins E, Pinho T, Vascoet al. Multiple coronary fistulae: characterization by multimodality imaging. Rev Port Cardiol. 2014 Feb;33(2):119-21.
- Gowda RM, Vasavada BC, Khan IA. Coronary artery fistulas: clinical and therapeutic considerations. Int J Cardiol. 2006 Feb 8;107(1):7-10.
- Knop GL, Madu E, Tulloch Reid E, et al. Off pump surgical epicardial closure of left anterior descending to pulmonary artery fistula. J Cardiothorac Surg. 2020 Oct 8;15(1):306.
- Van Loo I, Sonck J, Tanaka K, et al. Thoracoscopic off-pump closure of a large left circumflex coronary artery fistula: A novel minimally invasive approach. J Thorac Cardiovasc Surg. 2018 Oct;156(4):e159-e161.
- Hartnell GG, Jordan SC. Balloon embolisation of a coronary arterial fistula. Int J Cardiol. 1990 Dec;29(3):381-3.
- Kabbani Z, Garcia-Nielsen L, Lozano ML, et al. Coil embolization of coronary artery fistulas. A single-centre experience. Cardiovasc Revasc Med. 2008 Jan-Mar;9(1):14-7.
- Syed MI, Kalweit WH, Shaikh A. Microcoil embolization for treatment of a right coronary arteriovenous fistula. J Interv Cardiol. 2003 Aug;16(4):347-50.
- Sunkara A, Chebrolu LH, Chang SM, et al. Coronary Artery Fistula. Methodist Debakey Cardiovasc J. 2017 Apr-Jun;13(2):78-80.
Authors:
Valeria Pierluissi Rivera, M.D.
Internal Medicine Resident
University of South Alabama
Mobile, AL
Bassam Omar, M.D., Ph.D.
Professor of Cardiology
University of South Alabama
Mobile, AL